 By Tony Collins
By Tony Collins
Written evidence the Department for Work and Pensions submitted to an FOI tribunal – but did not want published (ever) – reveals that there was an internal “lack of candour and honesty throughout the [Universal Credit IT] Programme and publicly”.
It’s the first authoritative confirmation by the DWP that it has not always been open and honest when dealing with the media on the state of the Universal Credit IT programme.
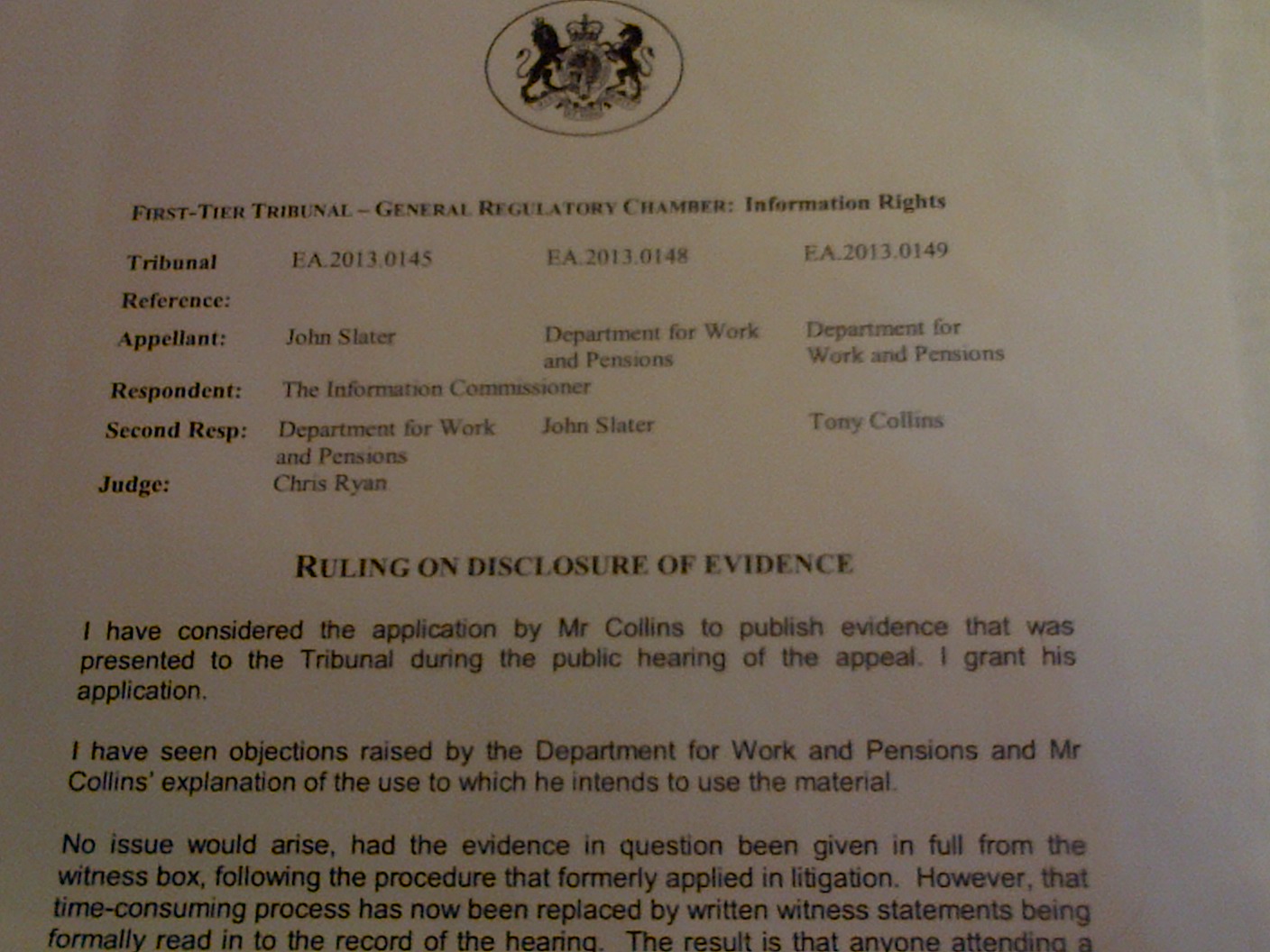
FOI tribunal grants request to publish DWP’s written submission
According to the DWP submission, senior officials on the Programme became so concerned about leaks that a former member of the security services was brought in to lead an investigation. DWP staff and managers were the subjects of “detailed interviews”. Employee emails were “reviewed”, as were employee access rights to shared electronic areas.
Staff became “paranoid” about accidentally leaving information on a printer. Some of the high-security measures appear still to be in place.
Unpublished until now, the DWP’s written legal submission referred, in part, to the effects on employees of leak investigations.
The submission was among the DWP’s written evidence to an FOI Tribunal in February 2016.
The Government Legal Service argued that the DWP’s written evidence was for the purposes of the tribunal only. It should not be published or passed to an MP.
The Legal Service went further: it questioned the right of an FOI Tribunal to decide on whether the submission could be published. Even so a judge has ruled that the DWP’s written evidence to the tribunal can be published.
Excerpts from the submission are here.
Analysis and Comment
The DWP’s submission gives a unique glimpse into day-to-day life and corporate sensitivities at or near the top of the Universal credit IT programme.
It reveals the lengths to which senior officials were willing to go to stop any authoritative “bad news” on the Universal Credit IT programme leaking out. Media speculation DWP’s senior officials do not seem to mind. What appears to concern them is the disclosure of any credible internal information on how things are progressing on Universal Credit IT.
Confidential
Despite multiple requests from IT suppliers, former government CIOs and MPs, for Whitehall to publish its progress reports on big IT-based change programmes (some examples below), all central departments keep them confidential.
That sensitivity has little to do with protecting personal data.
It’s likely that reviews of projects are kept confidential largely because they could otherwise expose incompetence, mistakes, poor decisions, risks that are likely to materialise, large sums that have been wasted or, worst of all, a project that should have been cancelled long ago and possibly re-started, but which has been kept going in its original form because nobody wanted to own up to failure.
 On this last point, former government CIO and permanent secretary Ian Watmore spoke to MPs in 2009 about how to fix government IT. He said,
On this last point, former government CIO and permanent secretary Ian Watmore spoke to MPs in 2009 about how to fix government IT. He said,
“An innovative organisation tries a lot of things and sometimes things do not work. I think one of the valid criticisms in the past has been when things have not worked, government has carried on trying to make them work well beyond the point at which they should have been stopped.”
Individual accountability for failure?
Oblivious to MPs’ requests to publish IT progress reports, the DWP routinely refuses FOI requests to publish IT progress reports, even when they are several years old, even though by then officials and ministers involved will probably have moved on. Individual accountability for failure therefore continues to be non-existent.
Knowing this, MPs on two House of Commons select committees, Public Accounts and Work and Pensions, have called for the publication of reports such as “Gateway” reviews.
This campaign for more openness on government IT projects has lasted nearly three decades. And still Whitehall never publishes any contemporaneous progress reports on big IT programmes.
It took an FOI campaigner and IT projects professional John Slater [@AmateurFOI] three years of legal proceedings to persuade the DWP to release some old reports on the Universal Credit IT programme (a risk register, milestone schedule and issues log). And he had the support of the Information Commissioner’s legal team.
 When the DWP reluctantly released the 2012 reports in 2016 – and only after an informal request by the then DWP secretary of state Stephen Crabb – pundits were surprised at how prosaic the documents were.
When the DWP reluctantly released the 2012 reports in 2016 – and only after an informal request by the then DWP secretary of state Stephen Crabb – pundits were surprised at how prosaic the documents were.
Yet we now know, thanks to the DWP’s submission, the lengths to which officials will go to stop such documents leaking out.
Understandable?
Some at the DWP are likely to see the submission as explaining some of understandable measures any government department would take to protect sensitive information on its largest project, Universal Credit. The DWP is the government largest department. It runs some of the world’s biggest IT systems. It possesses personal information on nearly everyone in Britain. It has to make the protection of its information a top priority.
Others will see the submission as proof that the DWP will do all it can to honour a decades-old Whitehall habit of keeping bad news to itself.
Need for openness
It’s generally accepted that success in running big IT-enabled change programmes requires openness – with staff and managers, and with external organisations and agencies.
IT-based change schemes are about solving problems. An introspective “good news only” culture may help to explain why the DWP has a poor record of managing big and successful IT-based projects and programmes. The last time officials attempted a major modernisation of benefit systems in the 1990s – called Operational Strategy – the costs rose from £713m to £2.6bn and the intended objective of joining up the IT as part of a “whole person” concept, did not happen.
Programme papers“watermarked”
The DWP’s power, mandate and funding come courtesy of the public. So do officials, in return, have the right to keep hidden mistakes and flawed IT strategies that may lead to a poor use – or wastage – of hundreds of millions of pounds, or billions?
The DWP’s submission reveals that recommendations from its assurance reports (low-level reports on the state of the IT programme including risks and problems) were not circulated and a register was kept of who had received them.
Concern over leaks
The submission said that surveys on staff morale ceased after concerns about leaks. IT programme papers were no longer sent electronically and were delivered by hand. Those that were sent were “double-enveloped” and any that needed to be retained were “signed back in”. For added security, Universal Credit programme papers were watermarked.
When a former member of the security services was brought in to conduct a leaks investigation, staff and mangers were invited by the DWP’s most senior civil servant to “speak to the independent investigator if they had any information”. This suggests that staff were expected to inform on any suspect colleagues.
People “stopped sharing comments which could be interpreted as criticism of the [Universal Credit IT] Programme,” said the submission. “People became suspicious of their colleagues – even those they worked closely with.
“There was a lack of trust and people were very careful about being honest with their colleagues…
“People felt they could no longer share things with colleagues that might have an honest assessment of difficulties or any negative criticism – many staff believed the official line was, ‘everything is fine’.
“People, even now, struggle to trust colleagues with sensitive information and are still fearful that anything that is sent out via email will be misused.
“For all governance meetings, all documents are sent out as password protected, with official security markings included, whether or not they contain sensitive information.”
“Defensive”
 Lines to take with the media were added to a “Rolling Brief”, an internal update document, that was circulated to senior leaders of the Universal Credit IT programme, the DWP press office and special advisors.
Lines to take with the media were added to a “Rolling Brief”, an internal update document, that was circulated to senior leaders of the Universal Credit IT programme, the DWP press office and special advisors.
These “lines to take” were a “defensive approach to media requests”. They emphasised the “positive in terms of progress with the Programme without acknowledging the issues identified in the leaked stories”.
This positive approach to briefing and media management “led to a lack of candour and honesty through the Programme and publically …”
How the DWP’s legal submission came about is explained in this separate post.
Were there leaks of particularly sensitive information?
It appears not. The so-called leaks revealed imperfections in the running of the Universal Credit programme; but there was no personal information involved. Officials were concerned about the perceived leak of a Starting Gate Review to the Telegraph (although the DWP had officially lodged the review with the House of Commons library).
The DWP also mentioned in its statement a leak to the Guardian of the results of an internal “Pulse” survey of staff morale – although it’s unclear why the survey wasn’t published officially given its apparent absence of sensitive commercial, personal, corporate or governmental information.
NPfIT
The greater the openness in external communications, the less likely a natural scepticism of new ways of working will manifest in a distrust of the IT programme as a whole.
The NHS’s National Programme for IT (NPfIT) – then the UK’s biggest IT programme costing about £10bn – was dismantled in 2011 after eight fraught years. One reason it was a disaster was the deep distrust of the NPfIT among clinicians, hospital technologists, IT managers, GPs and nurses. They had listened with growing scepticism to Whitehall’s oft-repeated “good news” announcements.
Ex-Government CIO wanted more openness on IT projects
When MPs have asked the DWP why it does not publish reports on the progress of IT-enabled projects, it has cited “commercial confidentiality”.
But in 2009, Ian Watmore (the former Government CIO) said in answer to a question by Public Account Committee MP Richard Bacon that he’d endorse the publication of Gateway reviews, which are independent assessments of the achievements, inadequacies, risks, progress and challenges on risky IT-based programmes.
“I am with you in that I would prefer Gateway reviews to be published because of the experience we had with capability reviews (published reports on a department’s performance). We had the same debate (as with Gateway reviews) and we published them. It caused furore for a few weeks but then it became a normal part of the furniture,” said Watmore.
Capability reviews are no longer published. The only “regular” reports of Whitehall progress with big IT programmes are the Infrastructure and Projects Authority’s annual reports. But these do not include Gateway reviews or other reports on IT projects and programmes. The DWP and other departments publish only their own interpretations of project reviews.
In the DWP’s latest published summary of progress on the Universal Credit IT programme, dated July 2016, the focus is on good news only.
But this creates a mystery. The Infrastructure and Projects Authority gave the Universal Credit programme an “amber” rating in its annual report which was published this month. But neither the DWP nor the Authority has explained why the programme wasn’t rated amber/green or green.
MPs and even IT suppliers want openness on IT projects
 In 2004 HP, the DWP’s main IT supplier, told a Work and Pensions Committee inquiry entitled “Making IT work for DWP customers” in 2004 that “within sensible commercial parameters, transparency should be maintained to the greatest possible extent on highly complex programmes such as those undertaken by the DWP”.
In 2004 HP, the DWP’s main IT supplier, told a Work and Pensions Committee inquiry entitled “Making IT work for DWP customers” in 2004 that “within sensible commercial parameters, transparency should be maintained to the greatest possible extent on highly complex programmes such as those undertaken by the DWP”.
The Work and Pensions Committee spent seven months investigating IT in the DWP and published a 240-page volume of oral and written in July 2004. On the matter of publishing “Gateway” reviews on the progress or otherwise of big IT projects, the Committee concluded,
“We found it refreshing that major IT suppliers should be content for the [Gateway] reviews to be published. We welcome this approach. It struck us as very odd that of all stakeholders, DWP should be the one which clings most enthusiastically to commercial confidentiality to justify non-disclosure of crucial information, even to Parliament.”
The Committee called for Gateway reviews to be published. That was 12 years ago – and it hasn’t happened.
Four years later the Committee found that the 19 most significant DWP IT projects were over-budget or late.

In 2006 the National Audit Office reported on Whitehall’s general lack of openness in a report entitled “Delivering successful IT-enabled business change”.
The report said,
“The Public Accounts Committee has emphasised frequently the need for greater transparency and accountability in departments’ performance in managing their programmes and projects and, in particular, that the result of OGC Gateway Reviews should be published.”
But today, DWP officials seem as preoccupied as ever with concealing bad news on their big IT programmes including Universal Credit.
The costs of concealment
The DWP has had important DWP project successes, notably pension credits, which was listed by the National Audit Office as one of 24 positive case studies.
But the DWP has also wasted tens of millions of pounds on failed IT projects.
Projects with names such as “Camelot” [Computerisation and Mechanisation of Local Office Tasks] and Assist [Analytical Services Statistical Information System) were cancelled with losses of millions of pounds. More recently the DWP has run into problems on several big projects.
“Abysmal”
On 3 November 2014 the then chairman of the Public Accounts Committee Margaret Hodge spoke on Radio 4’s Analysis of the DWP’s ‘abysmal’ management of IT contracts.”
1984
As long ago as 1984, the House of Commons Public Accounts Committee called for the civil service to be more open about its progress on major computer projects.
Today there are questions about whether the Universal Credit IT will succeed. Hundreds of millions has already been spent. Yet, as mentioned earlier, current information on the progress of the DWP’s IT programmes remains a state secret.
It’s possible that progress on the Universal Credit IT programme has been boosted by the irregular (but thorough) scrutiny by the National Audit Office. That said, as soon as NAO reports on Universal Credit are published, ministers and senior officials who have seen copies in advance routinely dismiss any criticisms as retrospective and out-of-date.
Does it matter if the DWP is paranoid about leaks?
A paper published in 2009 looks at how damaging it can be for good government when bureaucracies lack internal challenge and seek to impose on officials a “good news” agenda, where criticism is effectively prohibited.
The paper quoted the then Soviet statesman Mikhail Gorbachev as saying, in a small meeting with leading Soviet intellectuals,
“The restructuring is progressing with great difficulty. We have no opposition party. How then can we control ourselves? Only through criticism and self-criticism. Most important: through glasnost.”
Non-democratic regimes fear a free flow of information because it could threaten political survival. In Russia there was consideration of partial media freedom to give incentives to bureaucrats who would otherwise have no challenge, and no reason to serve the state well, or avoid mistakes.
The Chernobyl nuclear disaster, which occurred on April 26, 1986, was not acknowledged by Soviet officials for two days, and only then after news had spread across the Western media.
The paper argued that a lack of criticism could keep a less democratic government in power. But it can lead to a complacency and incompetence in implementing policy that even a censored media cannot succeed in hiding.
As one observer noted after Chernobyl (Methvin in National Review, Dec. 4, 1987),
“There surely must be days—maybe the morning after Chernobyl—when Gorbachev wishes he could buy a Kremlin equivalent of the Washington Post and find out what is going on in his socialist wonderland.”
Red team
 A lack of reliable information on the state of the Universal Credit IT programme prompted the then secretary of state Iain Duncan Smith to set up his own “red team” review.
A lack of reliable information on the state of the Universal Credit IT programme prompted the then secretary of state Iain Duncan Smith to set up his own “red team” review.
That move was not known about at the time. Indeed in December 2012 – at a point when the DWP was issuing public statements on the success of the Universal Credit Programme – the scheme was actually in trouble. The DWP’s legal submission said,
“In summary we concluded (just before Christmas 2012) that the IT system that had been developed for the launch of UC [Universal Credit] had significant problems.”
One wonders whether DWP civil servants kept Duncan Smith in the dark because they themselves had not been fully informed about what was going on, or because they thought the minister was best protected from knowing what was going on, deniability being one key Whitehall objective.
But in the absence of reliable internal information a political leader can lose touch completely, said the paper on press freedom.
“On December 21, 1989, after days of local and seemingly limited unrest in the province of Timi¸ Ceausescu called for a grandiose meeting at the central square of Bucharest, apparently to rally the crowds in support of his leadership. In a stunning development, the meeting degenerated into anarchy, and Ceausescu and his wife had to flee the presidential palace, only to be executed by a firing squad two days later.”
Wrong assumptions
Many times, after the IT media has published articles on big government IT-based project failures, TV and radio journalists have asked to what extent the secretary of state was responsible and why he hadn’t acted to stop millions of pounds being wasted.
But why do broadcast journalists assume ministers control their departments? It is usually more likely that ministers know little about the real risks of failure until it is too late to act decisively.
Lord Bach, a minister at DEFRA, told a House of Commons inquiry in 2007 into the failure of the IT-based Single Payment Scheme that he was aware of the risks but still officials told him that systems would work as planned and farmers would receive payments on time. They didn’t. Chaos ensued.
“I do think that, at the end of the day, some of the advice that I received from the RPA [Rural Payments Agency] was over-optimistic.”
 Another DEFRA minister at the time Lord Whitty, who was also party in charge of the Single Payment Scheme, told the same inquiry,
Another DEFRA minister at the time Lord Whitty, who was also party in charge of the Single Payment Scheme, told the same inquiry,
“Perhaps I ought also to say that this was the point at which I felt the advice I was getting was most misleading, and I have used the term ‘misleading’ publicly but I would perhaps prefer to rephrase that in the NAO terms …”
Even the impressive Stephen Crabb – who has now quit as DWP secretary of state – didn’t stand much of chance of challenging his officials. The department’s contracts, IT and other affairs, are so complex and complicated – there are bookcases full of rules and regulations on welfare benefits – that any new ministers soon find themselves overwhelmed with information and complexity.
They will soon realise they are wholly dependent on their officials; and it is the officials who decide what to tell the minister about internal mistakes and bad decisions. Civil servants would argue that ministers cannot be told everything or they would be swamped.
But the paper on press freedom said that in order to induce high effort within a bureacucracy, the leader needs “verifiable information on the bureaucrats’ performance”.
The paper made a fascinating argument that the more complacent the bureaucracy, the more aggressively it would control information. Some oil-rich countries, said the paper, have less media freedom than those with scarcer resources.
“Consistent with our theory, [some] non-democratic countries … have vast resources and poor growth performance, while the Asian tigers (South Korea, Taiwan, Hong Kong, and Singapore), while predominantly non-democratic in the 1970s and 1980s, have high growth rates and scarce natural resource.”
In an apparent opening up of information, the government in China passed a law along the lines of the U.S. Freedom of Information Act (“China Sets Out to Cut Secrecy, but Laws Leave Big Loopholes,” New York Times, Apr. 25, 2007). But was this law self-serving? It, and the launch of local elections, provided the central government with relatively reliable information on the performance of provincial bosses.
These stories from less democratic countries may be relevant in Britain because politicians here, including secretaries of state, seem to be the last to know when a big IT-based programme is becoming a disaster.
Bad news
Whtehall’s preoccupation with “good news only” goes well beyond the DWP.
T auditors Arthur D Little, in a forensic analysis of the delays, cost over-runs and problems on the development of a huge air traffic control IT project for National Air Traffic Services, whose parent was then the Civil Aviation Authority, which was part of the Department for Transport, referred to an “unwillingness to face up to and discuss bad news”.
Ministers helpless to force openness on unwilling officials?
Francis Maude came to the Cabinet Office with a reforming zeal and a sophisticated agenda for forcing through more openness, but the effects of his efforts began to evaporate as soon as he left office. Even when he was at the height of his power and influence, he was unable to persuade civil servants to publish Gateway reviews, although he’d said when in opposition that he intended to publish them.
His negotiations ended with central departments agreeing to publish only the “traffic light” status of big projects – but only after a minimum delay of at least six months. In practice the delay is usually a year or more.
Brexit
Brexit campaigners argue that the EC is undemocratic, that decisions are taken in Brussels in secret by unelected bureaucrats. But the EC is at least subject to the scrutiny, sometimes the competing scrutiny, of 29 countries.
Arguably Whitehall’s departments are also run by unelected bureaucrats who are not subject to any effective scrutiny other than inspections from time to time of the National Audit Office.
Yes Minister parodied Sir Humphrey’s firm grip on what the public should and should not be told. Usually his recommendation was that the information should be misleadingly reassuring. This was close enough to reality to be funny. And yet close enough to reality to be serious as well. It revealed a fundamental flaw in democracy.
Nowhere is that flaw more clearly highlighted than in the DWP’s legal submission. Is it any surprise that the DWP did not want the submission published?
If officials had the choice, would they publish any information that they did not control on any of their IT projects and programmes?
That’s where the indispensable work of the National Audit Office comes into the picture – but it alone, even with the help of the Public Accounts Committee, cannot plug the gaping hole in democracy that the DWP’s submission exposes.
These are some thoughts I am left with after reading the legal submission in the light of the DWP’s record on the management of IT-based projects …
- Press freedom and the free flow of information cannot be controlled in a liberal democracy. But does Whitehall have its own subtle – and not so subtle – ways and means?
- In light of the DWP’s track record, the public and the media are entitled to distrust whatever ministers and officials say publicly about their own performance on IT-related programmes, including Universal Credit.
- More worryingly, would the DWP’s hierarchy care a jot if the media and public didn’t believe what the department said publicly about progress on big projects such as Universal Credit?
- Is the DWP’s unofficial motto: Better to tell a beautiful lie than an ugly truth?
- AL Kennedy mentioned the “botched” Universal Credit programme when she gave a “point of view” on Radio 4 last week. Not referring specifically to Universal Credit she said facts can be massaged but nature can’t be fooled. A girder that won’t hold someone’s weight is likely to fail however many PR-dominated assurance reports have gone before. “Facts are uncompromising and occasionally grim. I wish they weren’t. Avoiding them puts us all at increased risk,” she said.
Excerpts from the DWP submission
Some Twitter comments on this post:
![]()
![]()
![]()
![]()